



Intresting Cases
In past decade biliary tract IPMN has been recognised as a unique type of mucinous papillary neoplasm and counterpart of pancreatic IPMN . These are differentiated from biliary cystadenoma by absence of ovarian stroma on histology ( typical of cystadenoma) and are at a higher risk of progression to invasive malignancy compared to cystadenoma . The type I Intrahepatic variant presents unique diagnostic challenges. We had 2 such cases interesting cases in last 2 months
Case 1 60 yr male presented with abdominal discomfort MRCP showed a Rt liver cystic lesion with biliary communication and a dilated Rt bile duct. Ca 19-9 was 600 iu/ ml . In view above features we proceeded with a right hepatectomy . Dilated Bile ducts were divided at confluence and margins sent for frozen. Histology was IPMN BTwith low grade dysplasia..
Case 65 yr old female presented with obstructive jaundice .MRI and CT revealed dilated dilated biliary tree with cyst at porta . Spy scopy revealed papillary growth at confluence extending to Rt side. Initially the extrahepatic biliary tree was resected and revealed a papillary mass extending into Right duct. On table the exophytic cyst wall was excised it was filled with mucionous material and frozen showed invasive malignancy in cyst wall. Rt hepatectomy with resection of extrahepatic bile duct was performed. HIstology revealed IPMN BT with focus of invasive malignancy in cyst wall.
Linkedin | Facebook | Instagram | Twitter | Pintrest | Youtube

Intresting Images
PV reconstruction With splenic vein ligation in whipples PD. 50 yr female with lower CBD cholangiocarcinoma with involvement of SMV PV junction. Traditionally in such cases we keep the SMV SV confluence intact for anastomosis ( technique shared previously) In This patient after resection as the length of involvement was more primary anastomosis lead to angulation and narrowing of confluence.
Rather than use a graft we decided to ligate splenic vein and do primary portal vein to SMV anastomosis. Risk of splenic vein ligation is left sided portal hypertension with varices and risk of gastric congestion with gastric bleeding ,DGE in post op . In this patient we decided to ligate the splenic artery at origin to mitigate risk of portal hypertension especially as left gastric was opening into splenic vein rather than portal vein . Patient had an unevetful recovery by day 7 with no DGE , hypersplenism and follow up UGIE at 2.5 months shows no varices.
Splenic artery ligation is a useful to mitigate the problems of splenic vein ligation during PV reconstruction in whipples esp when left gastric is not opening into portal vein
Linkedin | Facebook | Instagram | Twitter | Pintrest | Youtube



Intersting case:
complex GI reconstructions .52 yr old lady 5 yrs back cby a rectum and ascending colon villous Adenoma underwent Neoadjuvant RT followed low anterior resection with ileo cecal resection with a covering ileostomy followed by ileostomy closure. 2 yrs ago she underwent a hybrid IPom for incisional hernia. Advised surveillance endoscopy but Lost to follow up for 2 years.
Now she presented with descending colon growth with an enterocolic fistula presenting with severe diahhorea and 20 kg weight loss. We performed jejunal resection ( fistula site) with an ileal segmental resection ( as both loops were stuck at fistula site) . The plan for total colectomy and ileostomy was changed to left hemicolectomy as we felt an terminal ileostomy with reduced small bowel length May impair her nutritional recovery for chemo and subsequent life. As this was the second left sided resection after LAR . A covering transverse colostomy was added.
Now pt has 1. Jejunal RA site 2. Ileal RA site 3 old ileostomy closure 4 old ilececal RA site 5 present left hemicolectomy 6. Old LAR 7. Transverse loop colostomy that will be closed in 2 months. Total of 7 anastomosis.
Linkedin | Facebook | Instagram | Twitter | Pintrest | Youtube
Intresting Images
Utility of ICG in ca Rectum lap LAR. ICG injection helps us confidently identify the proximal transection in mid- sigmoid after IMA ligation in this morbidly obese patient.
Especially useful in lap LAR in obese pts where we cannot clearly make out branching pattern and pulsations. Also very useful colon pull up , gastric pull up to delineate conduit vascularity and lap liver resections to mark transection plane. Can be used in cholecystectomy also to avoid bile duct injury.
Linkedin | Facebook | Instagram | Twitter | Pintrest | Youtube

Intresting Images
Intersting Images: Acute superior mesenteric arterial ischemia mostly present with gangrene gut with a very narrow window for successful re-vascularisation. This was one 32 year old referred with SMA occlusion with clinical features of gangrene gut. We immediately took her for an emergency laparotomy in the middle of night . at surgery 30 cm of jejunum was ischemic with rest of the bowel showing borderline vascularity.
With our past experience of couple of elective Aortomesenteric bypass for chronic ischemia and considering the logistics and 3-4 hr delay in arranging vascular stenting with risk of further Howe ischemia we decided on table to proceed with an aortic mesenteric bypass with 10 mm PTFE graft ( normally we use a ringed PTFE normally but in emergency not available) . The bowel improved markedly immediately and as were happy about vascularity we decided to go for a primary anastomosis with the option of a re look in case of leak or clinical worsening.
The relook was deferred as the patient had a smooth recovery post op. Her echo heart and vasculitic workup was negative Patient was discharged on anti platelet and acitrom and is planned for prothrombitic workup at 6 months follow up
Linkedin | Facebook | Instagram | Twitter | Pintrest | Youtube
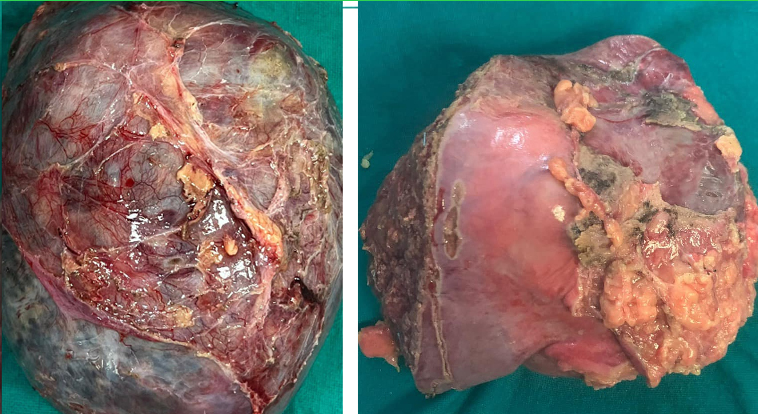
Hemmorgagic complications of liver tumor
Hemmorgagic complications of liver tumor . Liver Tumor bleeds are usually managed by angio embolisation. But in selected stable patients surgery can provide definitive control of both bleed and tumor. We saw two such cases in last month.
Case1. Cystic lesion of liver with intracystic arterial bleed after aspiration attempted outside . Patient presented with anemia high grade fever and severe right upper quadrant pain. CT image (case1) shows active contrast extravasating. As she was hemodynamically stable she was taken up for definitive resection. Histology revealed neuroendocrine neoplasm of liver grade 1. dotatac pet after surgery was clear.
2. Adult male with a sub capsular tumor rupture and hematoma presented with anemia. CT showed left lobe SOL with large subcapsular hematoma. Patient underwent a left hepatectomy. Histology was suggestive of well differentiated HCC.
Linkedin | Facebook | Instagram | Twitter | Pintrest | Youtube




Post cholecystectomy bile duct injury with type IV BBS
Post cholecystectomy bile duct injury with type IV BBS ( trifurcation anatomy with Rt anterior and posterior separated) managed by ERCP stenting outside for past 5 months. Both endoscopic stents were on Rt side and pt had reccurant episodes of cholangitis with multiple cholangiolytic abscesses on Rt side. Underwent 5 times stent changes and 3 PCDs and was on IV antibiotics for 80 percent of time in past 5 months. No evidence of vascular injury. We did a right hepatectomy with a left hepaticojejunostomy. Struggled for 14 days had cabdidial sepsis ( blood culture on day 2) needing anudulafungin with huge costs. Still in hospital .
Case 2. On same day we did another type IV BBS referred to us directly after injury . Sent home without any endoscopic stenting or PTBD and called after 3 months for surgery. He has no issue other than occasional pruritis in these 3 months. Simple hepaticojejunostomy with septoplasty discharged by day 4 . Just highlights the importance of choosing your biliary interventions carefully in complex HPB cases. We can just condemn them if we choose wrong.
Linkedin | Facebook | Instagram | Twitter | Pintrest | Youtube




Whipples for benign disease:
whipples is usually reserved for pancreatic and periampullary cancers. In selected cases of CP -complex head masses with suspicion of malignancy , triple obstruction or intractable pain whipples may be needed . This was one such patient chronic ethanolic abstinent since 2 years presented with debilitating pain for past 6 months with intermittent vomiting and 10 kg wt loss. CT showed large complex cystic mass 12x 10 cmwith duodenal biliary and pancreatic duct obstruction.
EUS guided aspiration cytology and Tumor market levels were negative for malignancy. Patient underwent a whipples PD . Though the surgery is difficult due to the severe inflammation and scarring secondary to reccurant inflammation the post op recovery is usually smooth. This patient is completely free from pain post surgery with good nutritional recovery. We have performed 7 whipples in CP for indications - Head mass suspicious of malignancy 4, trauma -1 ,large Pseudoaneurysm in head with bleed post angio mobilisation- 1 and revision surgery for persistent pain after LPJ-1, choledodchal cyst -1.
Linkedin | Facebook | Instagram | Twitter | Pintrest | Youtube




An interesting anecdote:
Post cholecystectomy bile duct injury with type IV BBS ( trifurcation anatomy with Rt anterior and posterior separated) managed by ERCP stenting outside for past 5 months. Both endoscopic stents were on Rt side and pt had reccurant episodes of cholangitis with multiple cholangiolytic abscesses on Rt side. Underwent 5 times stent changes and 3 PCDs and was on IV antibiotics for 80 percent of time in past 5 months. No evidence of vascular injury. We did a right hepatectomy with a left hepaticojejunostomy. Struggled for 14 days had cabdidial sepsis ( blood culture on day 2) needing anudulafungin with huge costs. Still in hospital .
Case 2 On same day we did another type IV BBS referred to us directly after injury . Sent home without any endoscopic stenting or PTBD and called after 3 months for surgery. He has no issue other than occasional pruritis in these 3 months. Simple hepaticojejunostomy with septoplasty discharged by day 4 . Just highlights the importance of choosing your biliary interventions carefully in complex HPB cases. We can just condemn them if we choose wrong.
Linkedin | Facebook | Instagram | Twitter | Pintrest | Youtube